Maple and Brett Belchetz, at the intersection of private, for-profit healthcare and MAiD
For many years, the same voices telling us we need more private healthcare have also been advocating for expansion of medical assistance in dying.

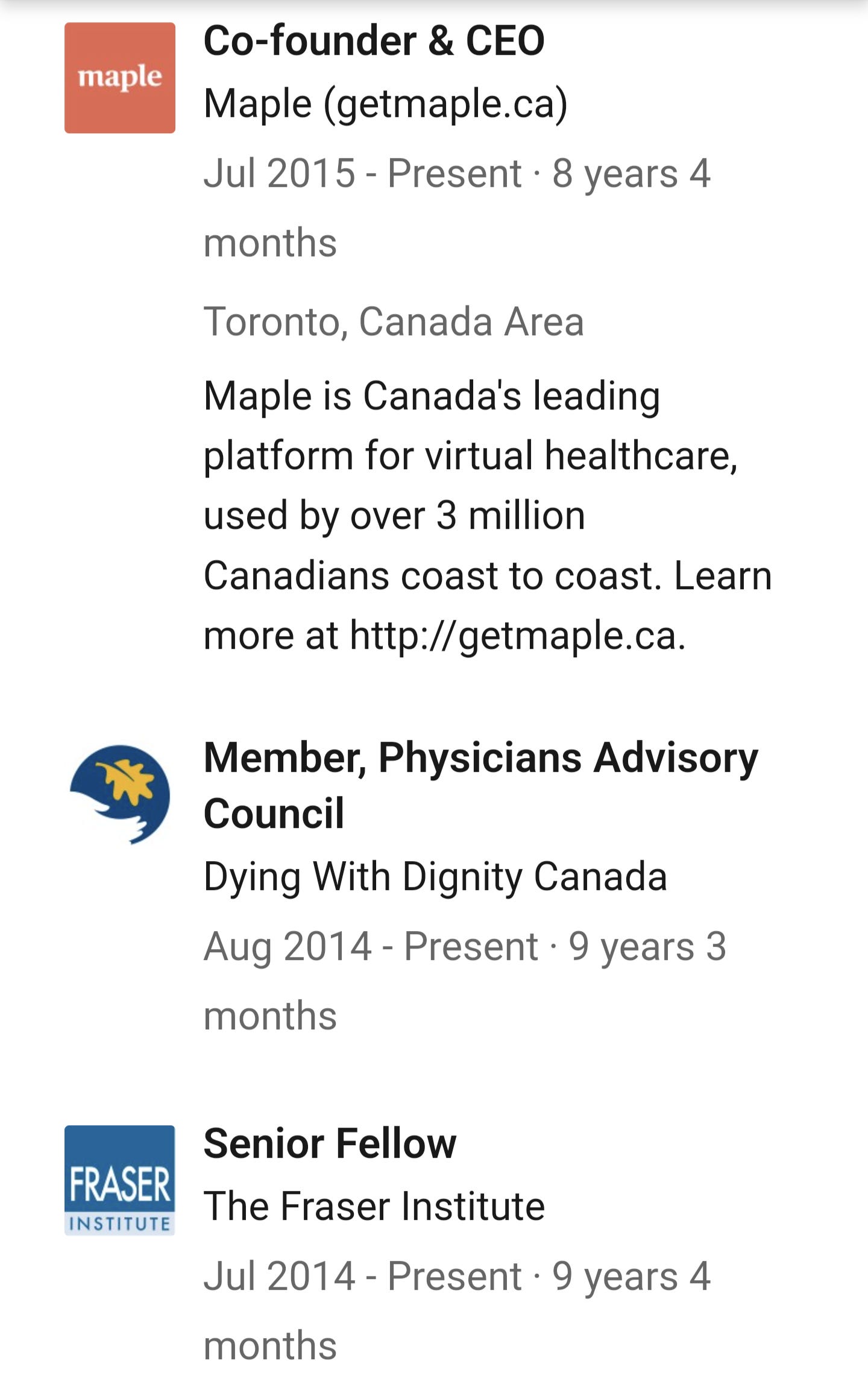
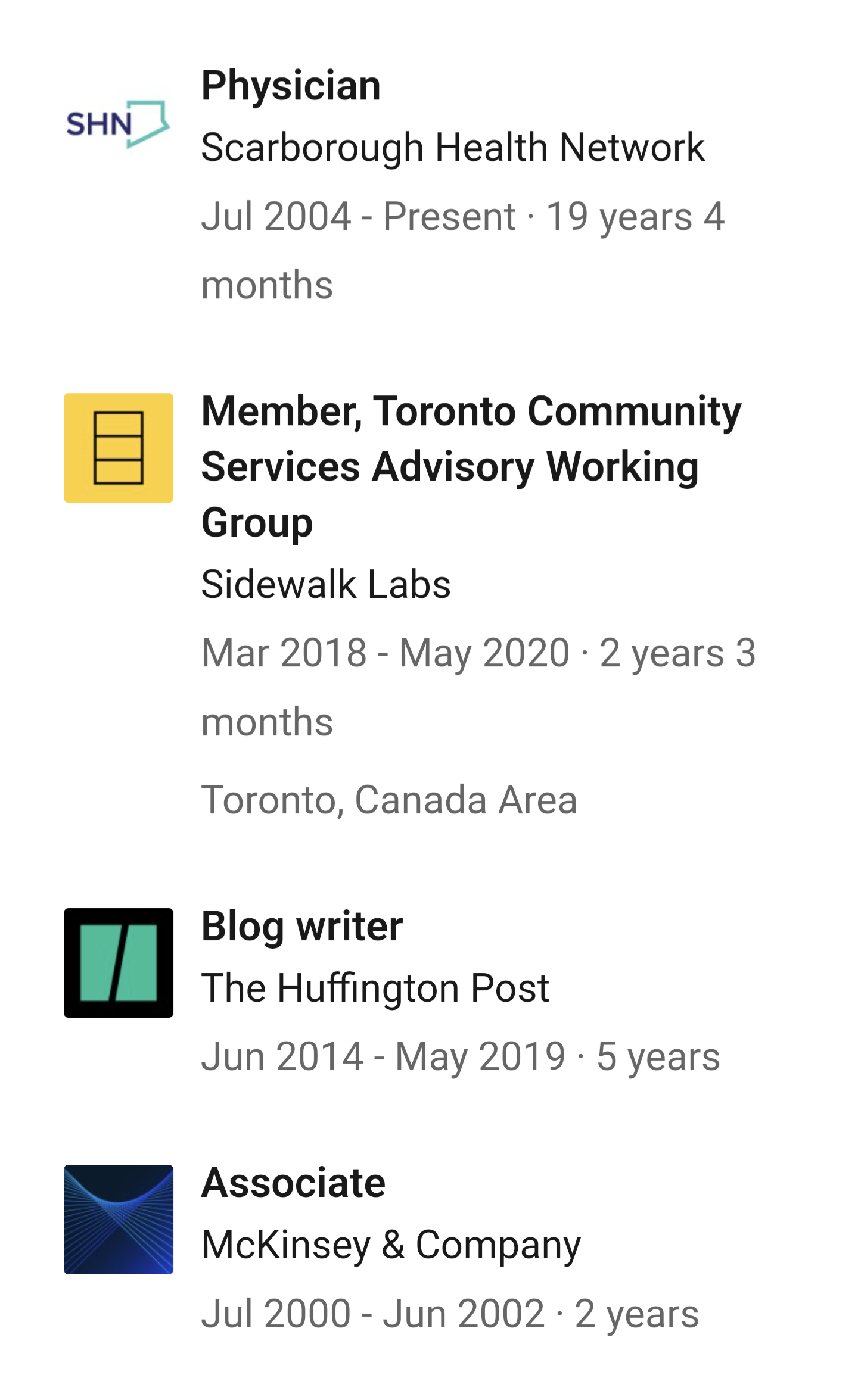
Dr. Brett Belchetz is a key figure in Canada’s increasingly privatized healthcare space, as CEO of private healthcare provider, Maple. As a former management consultant at McKinsey and a senior fellow of the Fraser Institute, it is unsurprising that Belchetz is a proponent of private healthcare, or keen to convince the public that for-profit care is superior - normalization of these positions has made Dr. Belchetz very rich, and set to become much richer.
Belchetz’s role in Canada’s legalization and expansion of medical assistance in dying may be more surprising.
As we wrote earlier this year, Galen Weston’s decades-long plan to privatize primary care in Canada under his ownership has been incredibly successful, despite flying under the radar for most Canadians. The pandemic provided the opportunity for a giant leap forward for Loblaws, Shoppers and Maple.
The timing of the pandemic couldn’t have been a bigger gift for Galen’s healthcare and profit ambitions, in many ways. He had already managed to get Doug Ford to drop the planned increase to the Ontario minimum wage, via a secret meeting right after Doug was elected, ensuring sky high profits when Loblaws was one of the only locations open for “essentials.”
By 2020, a few quarters into the pandemic, Loblaws invested $75 million in virtual health provider Maple Corporation, for whom the pandemic had already been a windfall. But Maple and Loblaws were already connected, as Shoppers Drug Mart was already invested in the company.
Setting the stage to privatize Canada’s much-beloved public healthcare system has been decades in the making. Canada’s media outlets have gone to great lengths to platform and position Belchetz as a “medical expert” - he is a regular guest on CTV and Global, and writes op-eds for Postmedia and The National Post - but there are two features of his background that never make it into his introduction or his biography.
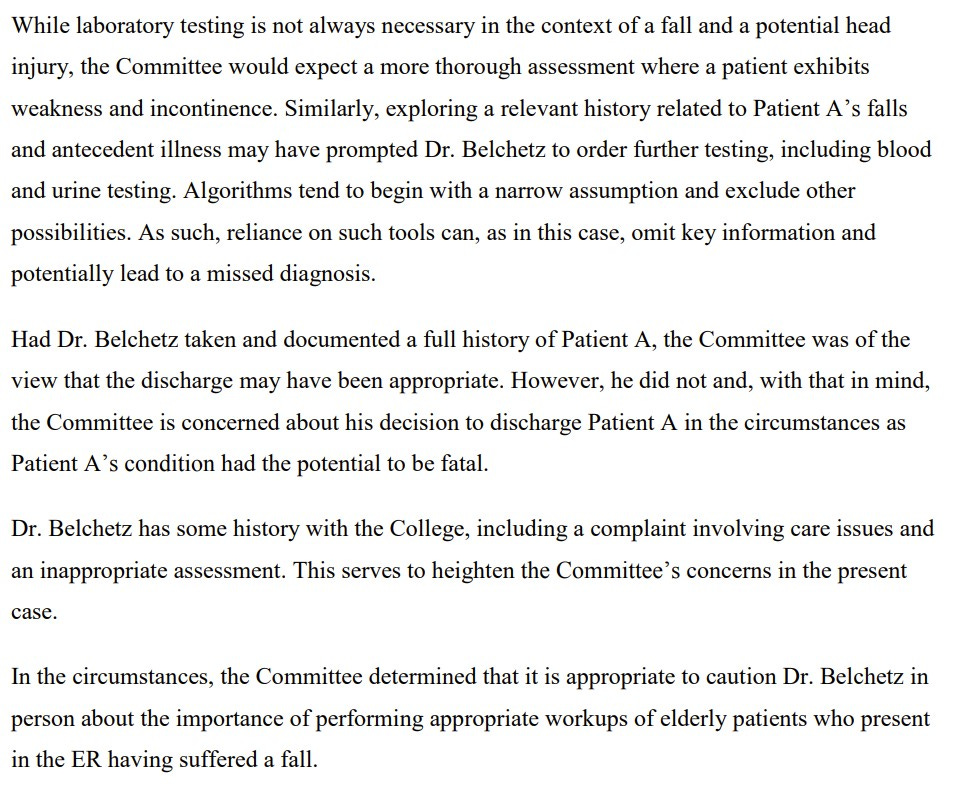
The first is Belchetz’ in-person caution from the College of Physicians and Surgeons of Ontario (CPSO) for improper work-up on an elderly patient presenting in the ER, after earlier complaints about his poor care and inappropriate assessments. (In the case for which he was cautioned, Belchetz failed to assess and order routine blood work or urine analysis for a elderly patient with head trauma, leading to an “inappropriate” discharge.)
The second area of Belchetz’ background that goes unmentioned is his association with Dying With Dignity. DWD is a Canadian lobby group which positions itself as a “national human-rights charity committed to improving quality of dying, protecting end-of-life rights, and helping people across Canada avoid unwanted suffering.” Incorporated as a Canadian charity in 1982, the organization has been relentlessly focused on removing legal barriers to medically-assisted death, and normalizing the idea of “right to die” in Canadian society through the media.
According to his LinkedIn profile, Belchetz has been a member of Dying With Dignity’s Physicians Advisory Council since 2014.
Indeed, that year he began publishing opinion pieces in the National Post to promote the idea of allowing hospital patients to choose AND (“a natural death”) rather than have CPR performed.
Thus, I recently stopped using the words “do not resuscitate” in all such discussions. For legal purposes, I retain the term on forms, but underneath, I write AND, and ask patients to focus instead on those three letters when they consider what they are requesting.
In the same paper, the same year, Belchetz lambasted the federal government for making “zero progress” on assisted death. As was common in Dying With Dignity’s messaging at the time, Belchetz focused solely on the need for physician-assisted death for “terminal disease with no hope of cure.”
The Hippocratic oath, taken by all physicians, offers as primary guidance to the profession the command “Never do harm to anyone,” and when it comes to assisted suicide, many in policy circles have interpreted this only in its most literal sense. I and many other physicians, however, believe that in cases where patients are suffering from a terminal disease with no hope of cure, where every moment of their existence consists of pain and suffering, and where they are clear minded enough to express a preference to no longer live in pain, to deny this clearly stated desire — to essentially torture them against their wishes — is in fact a grave form of harm. As Peter Goodwin, a prominent American physician once said, “As a physician, I resent the term ‘physician-assisted suicide.’ I have never felt I was assisting a suicidal patient, but rather aiding a patient with his or her end-of-life choice.”
The following year, in the same paper yet again, Belchetz wrote about the shortcomings of pain relief in palliative care, using data from a Dying With Dignity “poll” to support his point.
Meanwhile, this country and its doctors are more united on this issue than on almost any other matter of national debate, and contrary to Ms. Kay’s assertion, they do want the right to choice when it comes to assisted suicide. In a 2014 national survey, 84% of Canadians stated that they should have the right to choose physician-assisted suicide if they were suffering unbearably and clearly stated their desire for it. And in August of 2014, 91% of delegates to the Canadian Medical Association’s general council voted to amend the CMA’s policy to allow Canada’s doctors to perform such an act if it becomes legal in this country. There can be little debate that “no one wants euthanasia” is a grossly inaccurate statement in our nation.
That year, 2015, Dying With Dignity scored a major win in its three-decade campaign. The Supreme Court of Canada declared that an absolute prohibition on assisted suicide and euthanasia was unconstitutional. The following year parliament enacted C-14 permitting assisted suicide and euthanasia for individuals at end of life, terming it “Medical Assistance in Dying” or MAiD. That legal win was celebrated by Dying With Dignity, and Dr. Belchetz joined DWD’s CEO, Shanaaz Gokoll for a press conference to herald the new federal legislation.
When Canadians consider the value of MAiD and euthanasia, they generally think about individuals facing a terminal diagnosis or imminent death. This is indeed the impression Dying With Dignity has intended to leave with Canadians, with help from Canadian media. CBC, in particular, has run numerous “heartwarming” personal profiles over the last eight years of people opting for a “good death”, MAiD practitioners waxing philosophical about their role in ending lives, and advocacy to make sure MAiD deaths are not recorded by coroners as suicides.
Dying With Dignity’s lobbying did not end with the Supreme Court ruling of 2015, or the enactment of Bill C-14 in 2016. Indeed, some of its greatest success has come in the years since, with the rapid expansion of MAiD eligibility.
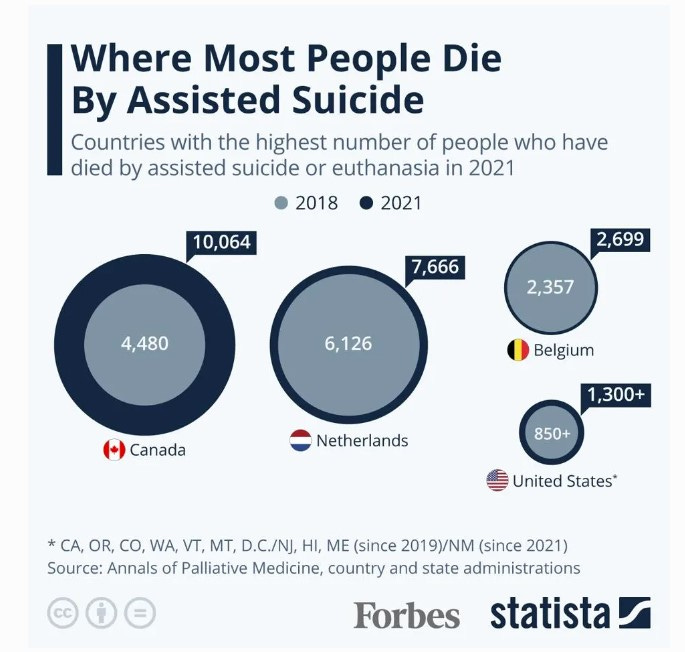
In 2021, parliament enacted Bill C-7 which expanded eligibility for MAiD to include people with disabilities who are not dying. That year, MAiD already accounted for 3.3% of deaths in Canada, with 10,064 deaths reported, surpassing all other jurisdictions internationally. By March of 2024, proposed legislation would make individuals eligible for MAiD if their only underlying condition is mental illness.
This rapid expansion of MAiD has coincided with a concerted effort in Ontario to reduce access to public healthcare, in order to hasten public acceptance for privatization. It has also coincided with an ongoing effort to cut social services.
In 2019, Doug Ford’s government cut half a billion dollars from the province’s two main income support programs, making deep cuts to Ontario Works and the Ontario Disability Support Program. By 2021, Ford’s government was actively privatizing social services, seeking to contract out “employment services” for people on social assistance to “better serve employers.” (One of the few eligible vendors is Maximus, a US company linked to Republican welfare cuts and “welfare to work” programs.) The message from the Ford government is clear, push people off income assistance and into the workforce.
For disabled people in Ontario, income assistance has increased very little in decades. In 2022, Ontario Disability Support Payment was increased by 5%, making it $14,700 a year for a single person, which is more than $5000 a year below $20,000 a year, recognized as the poverty line. According to Disability Without Poverty, 22% of Canadians live with a disability, but they make up 41% of Canadians who live in poverty.
Against this backdrop of increasing poverty and decreased access to care (particularly primary care) and social support for people with disabilities, the Canadian Association of MAiD Assessors and Providers (CAMAP) recommends that all those who “might qualify should be offered MAiD” as part of the “informed consent process.” No other country in the world has normalized assisted suicide as a potential first line therapeutic option to address suffering. Indeed, proactively offering MAiD is illegal in other jurisdictions where it is offered.
Speaking to the Standing Committee on Justice and Human Rights in November 2022, then federal minister of sports and persons with disabilities, Carla Qualthrough, asserted “it’s easier to access MAiD than it is to get a wheelchair.”
As I said, we know that in some places in our country, it's easier to access MAID than it is to get a wheelchair. That shouldn't be the case. That isn't what this law is about, but we wanted to make sure we spoke about the charter and the UN convention. I am committed to working with my provincial colleagues to make sure people are making the choice for reasons related to their circumstances, but not their social circumstances, not their lack of housing, not their lack of equipment, not their lack of employment.
Meanwhile, Dying With Dignity continues to assert that Canadians are not choosing MAiD due to poverty, lack of care, or inability to access supports like safe and affordable housing. In a 2022 Macleans article, DWD CEO, Helen Long, claimed it was “simply not true,” despite growing evidence to the contrary, and growing condemnation from around the world. Yet, she conceded that “shortfalls” in the system are leading Canadians to choose assisted death.
But should we deny those who are eligible the ability to access MAID because of those shortfalls in the system? Of course not. People should be able to make the choices that best align with their values, beliefs and needs at all stages of their life.
While DWD continues to normalize MAiD in Canada, internationally our approach has been condemned, particularly the planned expansion of eligibility for those who suffer only from mental illness. This planned expansion has also awoken mental health advocates and supporters domestically, who are beginning to join the disability community in raising the alarm.
Which brings us back to the interests of private medicine, specifically Maple and its omnipresent CEO, Brett Belchetz.

During the same years Belchetz was writing op-eds in support of MAiD, he was also writing (again in the National Post) about Canada’ public healthcare system. Unsurprisingly, given his own business interests, he was chastising Canada for throwing “endless billions into medicare” and offering arguments straight from (where else?) his colleagues at Fraser Institute.
Considering healthcare from an economic lens is Fraser Institute’s bread and butter, as is claiming that the ills of Canada’s healthcare system must be eased with more privatization. A brief overview of Fraser Institute’s research and commentary on healthcare shows quite clearly whose interests it considers, and those are the interests of oligarchs and capital.

Fraser Institute has been laying groundwork for privatization of Canadian healthcare and education since inception, funded and sometimes staffed by the Westons themselves. Galen’s cousin, Claudia Hepburn, is also a senior fellow at Fraser - her focus was “school choice”, Koch code for charter schools and private education. (Hepburn is quite popular - in addition to running a “charity” that lends money to immigrants, she also sits on boards of the LCBO, SickKids Foundation and the Weston Foundation.)
McKinsey, where Belchetz cut his teeth as a “management consultant” is also a forceful lever for healthcare privatization around the world. The influential consultancy (which played a key part in the ongoing diabolical COVID response among IDU-led countries all over the world) has been actively advising its clients to use the “gathering storms” as an opportunity to “reorder the healthcare industry”, which is code for making even more profit.
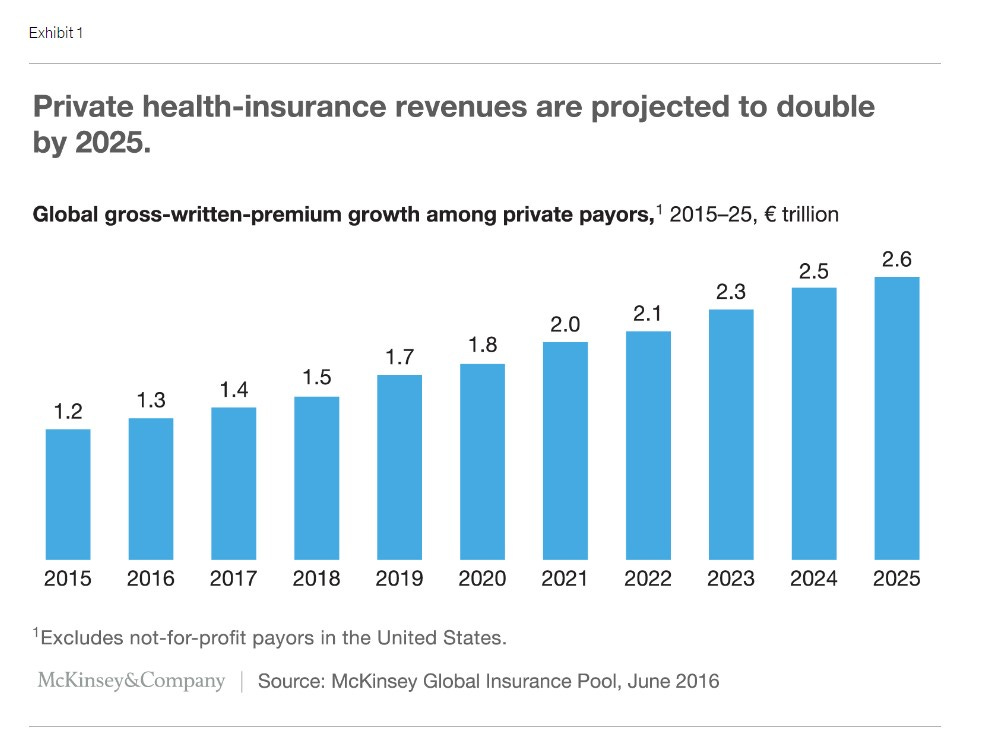
McKinsey sees private health insurance, particularly, as a huge growth opportunity. Naturally, Maple is a private health insurance company as well.
The intersection of MAiD advocacy and lobbying for private healthcare is not at all coincidental. Those who will profit most from private, for-profit healthcare have been carefully painting a rosy picture of healthcare under a private system for years and years. Having a large section of society (upwards of 20%) in need of care who cannot pay is troublesome for optics. People living with disabilities are also heavier users of the healthcare system, often dealing with chronic health issues. As a sector of society, disabled people pose a barrier to the aims of private healthcare, which is profit. It would certainly be beneficial to their growth and profitability to have fewer and fewer disabled people in our society.
Private capital took over Ontario’s long-term care system, beginning in the Mike Harris years, using many of the same “economic” arguments, from the same usual suspects. Many of the horrifying neglect stories from private long term care (of both staff and residents) have their roots in cost cutting and maximizing profit. Providing quality care costs money, and that cuts into profitability. Neglect saves money. Lobbying to reduce oversight and inspection (“removing gatekeepers”) increases profitability again.
As the pandemic has shown, and continues to show, those who care about accessible, quality healthcare must be prepared to fight back against incredibly well-financed corporations and individuals who seek to make our illness and disease a profit centre.
And this fight must include increased examination of the motives of the interests behind MAiD advocacy, which cannot be taken at face value.
Corruptario by Jordan Roberts & Friends is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.